



Study design
This study examines the socioeconomic, demographic, and cultural determinants of physical health development among Bangladeshi children aged 6 to 10 years. A two-stage sampling approach was employed to ensure representativeness.
In the first stage, four divisions—Dhaka, Chattogram, Mymensingh, and Rajshahi were randomly selected from the eight administrative divisions of Bangladesh. In the second stage, 33 elementary schools (17 government and 16 private institutions) were randomly chosen from these selected divisions to ensure diversity in school type and regional representation.
Children aged 6 to 10 years were included based on parental presence and consent from the selected schools. Only those whose parents were available at school on the day of data collection and who provided verbal consent participated in the study. Structured interviews were conducted with parents to gather information on socioeconomic status, demographic characteristics, and their children’s physical development.
Children who were absent on the survey day or whose parents did not provide consent were excluded from the study. This two-stage sampling strategy facilitated the inclusion of a diverse and representative sample while addressing logistical constraints in data collection.
Dependent variable
The dependent variable of this research is Children’s Physical Health, which is evaluated through six primary indicators, each rated on a 5-point Likert scale (Very Poor = 0, Poor = 1, Fair = 2, Good = 3, Very Good = 4). The indicators consist of the ability to Recover from Disease – which shows the child’s immune response and how quickly they recover from common illnesses. Restlessness – assesses the child’s tendency to be hyperactive, fidgety, or unable to remain calm. Sleeping Performance – encompasses the quality and length of sleep, along with how often the child wakes up during the night. Playing Intention – measures the child’s eagerness and willingness to participate in physical play. Self-control ability – reflects the child’s capacity to manage emotions and behaviours in social situations, and Motor Skills – reviews coordination and the capability to perform physical activities like running, jumping, and grasping objects. Together, these indicators offer a thorough perspective on children’s physical health.
Independent variable
Explanatory variables included a variety of socioeconomic and demographic parameters, such as gender (boy, girl), place of family residence (urban, rural), and house types, which were divided into three categories: single-family homes, apartments, and multi-family dwellings. Family types included joint families and nuclear families.
Among the demographic birth factors considered were the following: birth weight (less than 2.5 kg, 2.5–3.5 kg, > 3.5 kg), cesarean section delivery (yes, no), premature birth (yes, no), and breastfeeding status during the first six months (always breastfed, breastfed and formula-fed, always formula-fed). Additional factors included whether the mother took calcium-related drugs during pregnancy (yes, no), the mother’s nutritional status (poor, adequate), psychological stress during pregnancy (yes, no), current use of any family planning method (yes, no), and the mother’s age at the time of the child’s birth (less than 18, 18–25, 25–30, 30 + years).
Parents’ educational attainment was classified into four categories: illiterate, primary, secondary, and higher education. The father’s employment status was categorized into six types: government job, private job, daily labor, unemployed, remittance worker, and others. Monthly family income was divided into four ranges: less than 10,000, 10,000–20,000, 20,000–40,000, and more than 40,000. Religion was classified into two categories: Muslim and Hindu.
Data collection tool
After a comprehensive review of the existing literature, the authors developed a structured questionnaire for this study [23]. The questionnaire encompassed parental health during pregnancy, as well as challenges encountered by the child before and after birth, including early childhood illnesses and preterm birth. Trained interviewers conducted face-to-face interviews with parents to collect responses. Parental observations of their children served as the basis for assessing physical health development. The questionnaire was structured into three main sections. The first section included neonatal information such as the child’s age (number), gender (male or female), religion (Muslim, Hindu, or others), birth weight (< 2.5 kg, 2.5–3.5 kg, > 3.5 kg), early childhood disease (yes, no), premature birth (yes, no) and breastfeeding status in the first 6 months (always, breastfeed and formula milk, always formula milk). The second part provides information about parents’ socio-demographic traits and health status. The variables included in the second section were father’s age, mother’s age, number of household members, father’s and mother’s education (less than secondary level, secondary level, higher secondary level), father’s occupation (not employed, private service, government service, daily work, remittance worker), monthly family income (less than 10,000, 10,000–20,000, 20,000–40,000, and more than 40,000), family types (joint family, nuclear family), location of residence (urban, rural), mother’s age at childbirth (less than 18, 18–25, 25–30, 30+), maternal history of particular drug use throughout pregnancy (yes or no), Poor nutrition during pregnancy (No, Yes); Psychological stress during pregnancy (Yes, No). Parents’ education, occupation, family type (joint/nuclear), present residence, and monthly family income were all key characteristics utilized to assess socioeconomic status.
Finally, the socioeconomic status was divided into three categories: low, middle, and high. Mothers’ psychological stress levels during pregnancy were assessed based on their self-reports and use of antidepressants at the time. The third portion used the following domains to assess childhood physical health development outcomes: recovering from disease, rating the child’s restlessness, rating the child’s sleeping performance, rating the child’s playing intention, rating the child’s self-control ability and motor skill (picking up and holding tiny objects, standing, running, jumping, and so on).
Assessment of Children’s Physical Health Score (CPHSc)
The current study included six items to distinguish children’s physical health. Each item was coded with five levels: 0, 1, 2, 3 and 4. Where 0 means that the child’s physical health is very poor, 1 indicates poor physical health, 2 suggests medium physical health, 3 indicates good physical health, and 4 represents extremely good physical health. The CPHS considers the following items: Adding all six factors yields a total physical health score (TPHS) ranging from 2 to 24. The resulting TPHS was transformed into a score ranging from 0 to 1 by dividing the TPHS by 24 for each child. Let \(\:{V}_{ij}\) be the value of the \(\:{j}_{th}\:\)category of the \(\:{i}_{th}\) item responded by the parents of the children. Now the total physical health score (TPHS) for that child can be calculated by,
$${\rm TPHS } = \:\sum\:_{i}\sum\:_{j}{V}_{ij}$$
(1)
Where i = 1,2,3,. … … 0.6 and j = V = 0,1,2,3,4.
Now the Childhood Physical Health Score (CPHSc) can be calculated by the formula,
$$\:\text{C}\text{P}\text{H}\text{S}\text{c}\:=\:\frac{TPHS}{{TPHS}_{max}}\:=\:\frac{\sum\:_{i}\sum\:_{j}Vij}{{TPHS}_{max}}$$
Here \(\:{TPHS}_{max}\) can be obtained when j = 4 for all i.
The range of the CPHSc lies between 0 and 1, i.e., 0\(\:\le\:CPHS\le\:1\). CPHSc will be 0 when
j = 0 for all i, and 1 when j = 3 for all i.
This score is the Childhood Physical Health Score (CPHSc). The score tending from 0 to 1 indicates that the severity of physical health increased.
Sampling and data collection
A two-stage sampling technique was employed in this study to collect data on the physical health development of children. In the first stage, four administrative divisions of Bangladesh—Dhaka, Chattogram, Rajshahi, and Mymensingh—were randomly selected. According to the Annual Primary School Census 2021, Bangladesh had 118,891 primary-level educational institutions, including 65,566 government primary schools and 4,799 private primary schools.
In the second stage, 40 schools were randomly selected from these divisions, and written applications for data collection were submitted. Of these, 33 institutions granted permission for participation. The required sample size was determined using Cochran’s formula for a finite population, ensuring statistical validity and representativeness. The Cochran’s formula for sample size determination for the finite population is.
$$n = \frac{{n}_{0}}{1+\frac{{(n}_{0}-1)}{N}}$$
(2)
Where N is the size of the finite population, \(\:{n}_{0}\) is the sample size for an infinite population, and \(\:{n}_{0}\:\) be defined as
$$\:{n}_{0}=\frac{{z}^{2}pq}{{e}^{2}}$$
(3)
Here, z is the critical value of excepted confidence level, p is the proportion of a certain attribute presented in the population, q = 1-p, and e is the level of precision. Now if we consider 5% level of significance or 95% confidence interval, we have z = 1.96, considering the expected proportion of the study’s attribute is 50%, i.e., p = 0.5, q = 1 − p = 0.5, and e = 0.05. Putting all these values in Eq. (3), we can get \(\:{n}_{0}\) = 384.16\(\:\approx\:\)384. According to the Ministry of Primary and Mass education, the estimated number of primary school children in Bangladesh is 16,230,000. Hence, the population size for this study is N = 16,230,000. Now, using the value of N and \(\:{n}_{0}\), we have from Eq. (2)
$${\rm n}=\:\frac{384}{1+\frac{384-1}{16230000}} = 383.99\:\approx\:384 $$
(4)
The appropriate sample size for this study was determined to be 384 children. To account for potential issues such as incomplete responses and participant withdrawal, data collection efforts targeted 450 parents. Ultimately, complete responses were obtained from 401 participants, resulting in a response rate of 89.11%.
A team of trained professionals conducted face-to-face interviews with parents, who were informed that completing the questionnaire would take approximately 5–10 min. All collected data were recorded in an Excel spreadsheet for further analysis. The data collection period spanned from October 1, 2023, to March 1, 2024.
Since children were unable to provide information regarding their physical, socioeconomic, and demographic conditions, responses were obtained from their parents. A detailed illustration of the children’s physical health, as examined in this study, is presented in Fig. 1.
Statistical analysis
This study employed list-wise deletion to manage missing data, ensuring that all analyses were conducted using complete cases. The dependent variable, Child Physical Health Score (CPHS), is a numeric variable ranging from 0 to 1, where higher values indicate better physical health conditions. The Kolmogorov-Smirnov and Shapiro-Wilk tests confirmed the non-normality of the study variables (p < 0.05), as presented in Table 1. Due to the non-normal distribution of CPHS, traditional parametric regression methods, such as ordinary least squares (OLS), were deemed unsuitable. Instead, generalized linear models (GLMs) and other non-parametric approaches were applied to account for the data distribution.
To begin the analysis, a frequency distribution of all explanatory variables—covering children’s characteristics, parental socioeconomic status, and demographic traits—was generated to provide an overview of the dataset. Next, bivariate analyses were conducted using the Mann-Whitney U test and the Kruskal-Wallis H test. The Mann-Whitney U test was applied to assess differences in CPHS across binary categorical variables, while the Kruskal-Wallis H test was used for categorical variables with three or more groups [24]. The variables identified as important in the bivariate analysis were considered in the multivariate analysis.
Four generalized linear regression (GLM) models: generalized linear gamma regression (GLGR), generalized linear beta regression (GLBR) models, generalized log-normal regression (GLNR), and generalized exponential regression (GLER) have been applied to assess the significant impact of different socioeconomic and demographic variables on physical health. To determine the optimal model, the Akaike information criterion (AIC) and Bayesian information criterion (BIC) were calculated for each of the four [24]. The values of AIC (AIC: -488.9162) and BIC (BIC:-365.1034) in Table 2 were found to be the lowest for the GLNR model compared to the other three models, indicating that the generalized log-normal regression model is better than other models. The log-normal model allowed us to account for the positively skewed distribution of the dependent variable (child physical health scores), providing coefficients that are interpretable in terms of multiplicative effects. This is particularly useful for understanding proportional changes in health outcomes.
Hence, the results of the GLNR model have been extracted for this study and prepared the results accordingly. Kendall’s tau_b and Spearman’s rho correlation were used to analyze the link between physical health and other explanatory variables [24]. The statistical analysis was conducted using the software Statistical Package for Social Science (SPSS) v25 and R version 4.3.2.
Result
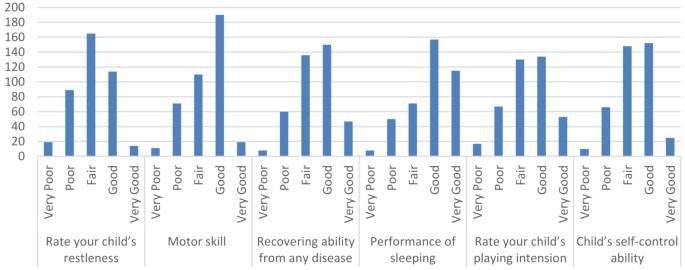
Figure 1 depicts the frequency of the physical health indicators used in this investigation. The figure shows that 190 children had good motor skills (47.4%), 150 demonstrated good disease recovery ability (37.4%), 157 showed good sleeping performance (39.2%) and 134 exhibited a positive child’s playing attitude (33.4%). Furthermore, the survey discovered that 152 (37.9%) of children exhibited high self-control abilities. These findings reflect the complexity of children’s physical health. While the majority of indicators yielded positive results, several places had slightly lower percentages. For instance, child restlessness 114 (28.4%) said that specific children required more care for their physical well-being.

Indicators of physical health
Characteristics of socioeconomic and demographic features
Tables 3 and 4 exhibit general frequency distribution tables generated to help understand the characteristics of the explanatory variables employed in this study. Regarding educational institutions, government schools received more students (68.1%) than private schools (31.9%). With 50.6% of girls and 49.4% of boys participating, the gender breakdown was almost equal. The division Chattogram accounted for the greatest percentage of children (30.2%). Participants’ religious makeup leaned more towards Muslims (82.8%) than Hindus (17.2%). Although there was variation in birth weight, the majority (52.9%) of the children were born with a weight between 2.5 and 3.5 kg. A significant majority of children (55.6%) had experienced early childhood illnesses, and nearly an equal proportion was born via cesarean Sect. (48.6%). Most children were not born prematurely (63.8%) and were nursed with formula milk for the first six months (56.4%). Furthermore, most parents gave their children supplemental food/milk on occasion (70.6%) and allowed them to play/go outside/meet friends on occasion (46.9%).
Table 4 shows that the majority of parents (74.1%) use a family planning approach. In terms of fathers’ education levels, only 16.2% (n = 65) have a primary level, 51.1% (n = 205) have secondary education, and 32.7% (n = 131) have further education. Table 4 reveals that 13.2% (n = 53) of the mothers had a higher education. The father’s occupations varied, with a significant presence in private (32.2%) and government jobs (23.2%). Monthly family income distribution ranged from less than 10k (5.5%) to 20k-40k (51.6%). The most frequent kind of housing was single-family dwellings (43.9%), followed by apartments (26.2%) and multi-family homes (29.9%). Urban areas were slightly more prevalent (59.4%) than rural regions (40.6%). The maternal age at childbirth varied, with a considerable proportion falling between the 18–25 age group (59.6%). Many children (n = 215, 53.6%) belong to nuclear families, whereas 46.4% (n = 186) live in joint households. The findings revealed that 52.0% (n = 209) of mothers had inadequate nutrition, and 66.7% (n = 268) experienced psychological stress during pregnancy. Table 4 also showed that 63.4% (n = 255) of pregnant women took calcium-related medications.
Bivariate analysis of the significant mean difference
Table 5 represents the results of bivariate analysis exploring the association or significant mean rank or median difference of physical health among different categories of the explanatory variables. The Mann-Whitney U tests demonstrate no significant differences in the median scores of CPHSc between school types (Mann-Whitney U = 16899, p > 0.05) and religion (Mann-Whitney U = 9796, p > 0.05). However, gender (Mann-Whitney U = 17337, p < 0.05) and early childhood disease (Mann-Whitney U = 15134, p < 0.05) emerge as significant factors associated with children’s physical health. Specifically, premature birth (Mann-Whitney U = 15390, p < 0.05), mother’s poor nutrition (Mann-Whitney U = 17192, p < 0.05), psychological stress during pregnancy (Mann-Whitney U = 15066.5, p < 0.05) also demonstrates significance in influencing physical health outcomes. Conversely, variables such as child’s delivery by caesarean section, family planning method, type of place of residence and family type show no significant associations with physical health.
In addition to the Mann-Whitney U test, the Kruskal-Wallis H test for testing the significant mean rank difference of CPHSc has been calculated and presented in Table 6. A significant difference is found between the children who have the opportunity to play or go outside or meet with friends (Kruskal-Wallis H = 10.824, P < 0.05), and the highest mean physical health score was observed in the children who were always given an opportunity to play/going outside/meeting with friends (0.6239\(\:\pm\:0.14700)\). Given child supplementary food/milk (Kruskal-Wallis H= 6.309, P<0.1) and the division (Kruskal-Wallis H= 12.326, P < 0.05) were found to be significant with physical health outcome. Furthermore, significant disparities are observed based on the father’s education levels (Kruskal-Wallis H = 14.326, P< 0.05) and fathers’ occupation (Kruskal-Wallis H= 11.177, P< 0.05) with higher-educated fathers and fathers who do private jobs correlating with higher physical health scores. Additionally, monthly family income (Kruskal-Wallis H= 28.517, P < 0.05) and the type of house (Kruskal-Wallis H= 6.012, P < 0.05) also exhibit significant associations with physical health outcomes, with lower-income households and individuals living in multi-family homes reporting lower physical health scores. Moreover, the table showed that the mother’s age at the time of birth of that child was also significant (Kruskal-Wallis H= 8.844, P < 0.05) with the score of physical health, with individuals born to mothers aged less than 18 showing lower physical health scores (0.5524\(\:\pm\:0.14149)\:\)compared to other age groups.
Table 7 shows a positive correlation coefficient between physical health scores and several demographic variables, including the child’s age, the father’s age, the mother’s age, and the number of household members. For instance, the positive coefficients suggest that with the increase in the parent’s age, the child’s physical health score also increases.
Impacts of neonatal, parental, socioeconomic and demographic factors on physical health
Table 8 illustrates the impact of socioeconomic and demographic factors on children’s physical health development. Early childhood disease shows a significant negative impact on physical health (OR: 0.9537, p = 0.000769), suggesting that children with early childhood diseases are about 4.63% less likely to have good physical health compared to those without such diseases. Infrequent opportunities for outdoor play also negatively impact physical health. Specifically, children who sometimes (OR: 0.9644, p = 0.025740) or seldom (OR: 0.9451, p = 0.007235) have the chance to play outside are respectively 3.56% and 5.49% less likely to have good physical health, compared to children who always play outside. The influence of gender seems to be minor but statistically significant. compared to boys, to be in better physical condition (OR: 0.9693, p = 0.025684). Additionally, children from the Rajshahi division have better physical health outcomes, being 1.05 times more likely (OR: 1.0496, p = 0.021429) to be in good health compared to children from other divisions. Moreover, income has a significant impact on physical health. Children from lower income families are roughly 7.53% less likely than those from families with higher incomes to be in good physical health (OR: 0.9247, p = 0.015046). Furthermore, providing supplementary food sometimes (OR: 1.0583, p = 0.001819) or seldom (OR: 1.0605, p = 0.026123) significantly improves children’s physical health, with these children being about 5.83% and 6.05% more likely, respectively, to have good physical health compared to those who are never provided supplementary food.
link