



Global incidence and prevalence rates of brain and CNS cancers
In 2021, the ASIR of brain and CNS cancers was 4.28 (95% UI: 3.71 to 4.88) per 100,000 population, representing an increase from 3.75 (95% UI: 3.21 to 4.21) in 1990 (Table 1). Similarly, the global ASPR rose from 8.66 (95% UI: 7.55 to 9.53) to 12.01 (95% UI: 10.54 to 13.52) per 100,000 over the same period. The EAPC values of 0.44 (95% CI: 0.4 to 0.49) for incidence and 1.18 (95% CI: 1.12 to 1.24) for prevalence indicate a steady upward trajectory throughout the 32-year study period. However, joinpoint regression analysis revealed important recent trend changes that challenge this apparent steady increase. Most notably, both incidence and prevalence showed significant recent declines, with incidence decreasing by −0.72 from 2018 to 2021 and prevalence declining by −0.85 during the same period (Table S1–S2). This recent downturn represents a notable shift from the significant increases observed in the preceding period (2003–2018 for incidence: 0.44; 2004–2018 for prevalence: 1.17).
When analyzed by sex, males consistently exhibited higher disease burden than females. In 2021, males had 190,130 new cases with an ASIR of 4.72 (95% UI: 3.68 to 5.76) compared to 167,353 new cases with an ASIR of 3.88 (95% UI: 3.43 to 4.35) for females (Table 1, Fig S1A). The EAPC values for incidence were 0.42 (95% CI: 0.38 to 0.47) for males and 0.47 (95% CI: 0.43 to 0.51) for females. The temporal analysis demonstrated that both sexes experienced significant recent declines in incidence during 2018–2021, though the magnitude differed substantially between males (−0.77) and females (−0.53) (Table S1). This contemporary downturn contrasts notably with the preceding growth phase, where females exhibited a more consistent upward trajectory (0.43 from 1997 to 2018) while males displayed greater temporal variability. Prevalence patterns showed similar sex differences, with males having 490,044 cases (ASPR: 12.28, 95% UI: 9.72 to 15.05) and females having 485,235 cases (ASPR: 11.76, 95% UI: 10.48 to 13.28) in 2021. The EAPC values for prevalence were 1.09 (95% CI: 1.03 to 1.15) for males and 1.28 (95% CI: 1.21 to 1.34) for females (Table 1, Fig S1B).
Examination across SDI quintiles revealed substantial disparities. High SDI regions reported the highest rates with an ASIR of 6.38 (95% UI: 6.08 to 6.64) and ASPR of 26.10 (95% UI: 24.84 to 27.19) in 2021, both having increased notably since 1990 (Table 1, Fig S1C-F). Remarkably, joinpoint analysis revealed that High SDI regions experienced the most pronounced recent decline, with incidence decreasing by −1.77 during 2018–2021 (Table S1). This sharp recent decrease contrasts markedly with the increases observed in the preceding period (2004–2018: 0.62), suggesting a significant epidemiological transition in the most developed regions. In contrast, low SDI regions had the lowest rates with an ASIR of 1.43 (95% UI: 1.00 to 1.82) and ASPR of 2.53 (95% UI: 1.76 to 3.24). When comparing age groups, the highest incidence and prevalence were observed in older populations, with rates increasing progressively with age (Fig S2, Table S3).
Global mortality and DALYs rates of brain and CNS cancers
The global ASMR remained relatively stable over the study period, with a slight increase from 3.04 (95% UI: 2.58 to 3.45) per 100,000 in 1990 to 3.06 (95% UI: 2.62 to 3.50) in 2021 (Table 2). Concurrently, the ASDR decreased from 119.88 (95% UI: 99.23 to 137.57) to 107.91 (95% UI: 91.74 to 125.59) per 100,000, with an EAPC of −0.37 (95% CI: −0.63 to −0.12). The segmented trend analysis illuminated notable recent improvements across both mortality and disability metrics. The 2018–2021 period witnessed substantial mortality reductions (−0.86) alongside even more dramatic decreases in DALYs (−1.21) (Table S4-S5). This accelerated improvement trajectory represents a marked departure from the more gradual progress characterizing earlier periods.
The mortality burden showed notable sex differences, with males experiencing higher rates. In 2021, the ASMR for males was 3.54 (95% UI: 2.75 to 4.32) compared to 2.62 (95% UI: 2.31 to 2.92) for females (Table 2, Fig S3 A). The EAPC values for mortality were 0.03 (95% CI: −0.02 to 0.09) for males and − 0.03 (95% CI: −0.08 to 0.02) for females. The DALYs burden followed a similar pattern to mortality, with males having an ASDR of 122.96 (95% UI: 93.65 to 157.33) and females having 93.46 (95% UI: 82.86 to 104.06) per 100,000 (Table 2, Fig S3B). EAPC values were − 0.37 (95% CI: −0.41 to −0.33) for males and − 0.37 (95% CI: −0.47 to −0.34) for females.
Analysis by SDI quintile revealed notable disparities in mortality and DALYs. High-middle SDI regions had the highest ASMR at 3.94 (95% UI: 3.36 to 4.51) per 100,000 in 2021, followed by high SDI at 3.54 (95% UI: 3.36 to 3.68), middle SDI at 3.02 (95% UI: 2.45 to 3.65), low-middle SDI at 2.08 (95% UI: 1.68 to 2.62), and low SDI regions at 1.33 (95% UI: 0.93 to 1.69) in 2021 (Table 2, Fig S3 C). From 1990 to 2021, high SDI regions showed a declining trend in mortality with an EAPC of −0.17 (95% CI: −0.51 to 0.17), while low-middle SDI regions experienced the largest increase with an EAPC of 0.88 (95% CI: 0.68 to 1.09). Joinpoint regression analysis revealed that high SDI regions experienced fluctuating mortality trends with periods of both increase and decrease, ultimately showing a pronounced decline in the most recent period (Table S4 and S5). For DALYs, high-middle, high, and middle SDI regions showed the substantial decreases with EAPCs of −0.68 (95% CI: −0.95 to −0.40), −0.43 (95% CI: −0.75 to −0.10), and − 0.40 (95% CI: −0.63 to −0.18), respectively, while low-middle SDI regions experienced an increase with an EAPC of 0.68 (95% CI: 0.47 to 0.90) (Table 2, Fig S3D-F). When examining age distributions, mortality and DALYs rates were mainly among individuals aged 60 years and above, highlighting the substantial burden of brain and CNS cancers in older populations (Fig S4, Table S6).
Geographical distribution of incidence, prevalence, mortality, and DALYs
Considerable geographical variation was observed in the burden of brain and CNS cancers in 2021. Norway recorded the highest ASIR at 14.96 per 100,000 (95% UI: 13.93 to 16.07), while Gambia had the lowest at 0.14 per 100,000 (95% UI: 0.09 to 0.19) (Fig. 1A, Table S3). The EAPCs for incidence rates showed diverse patterns globally, with the largest increase observed in Turkmenistan (7.44, 95% CI: 6.35 to 8.54) and the largest decrease in Greenland (−1.29, 95% CI: −1.48 to −1.11) (Fig. 1B, Table S3). The geographical distribution of prevalence rates followed a similar pattern to that of incidence rates (Fig. 1C, Table S3), with widespread increases in the EAPCs, particularly in Ecuador (7.69, 95% CI: 5.66 to 9.77), and Turkmenistan (7.51, 95% CI: 6.53 to 8.50) (Fig. 1D, Table S3).

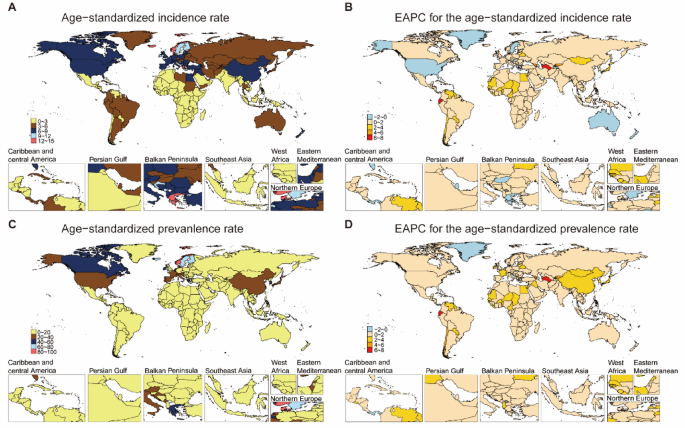
The Age-standardized Incidence and Prevalence Rate of Brain and CNS Cancers in 204 Countries and Territories. (A) The ASIR of brain and CNS cancers in 2021. (B) The EAPC of ASIR of brain and CNS cancers from 1990 to 2021. (C) The ASPR of brain and CNS cancers in 2021. (D) The EAPC of ASPR of brain and CNS cancers from 1990 to 2021. ASIR age-standardized incidence rate, ASPR age-standardized prevalence rate, EAPC estimated annual percentage change.
For mortality, Montenegro reported the highest rate at 7.77 per 100,000 (95% UI: 6.11 to 10.25), while Gambia again had the lowest at 0.12 per 100,000 (95% UI: 0.08 to 0.16) (Fig. 2A, Table S6). The EAPCs for mortality rates showed heterogeneous trends globally, with notable increases in Turkmenistan (7.30, 95% CI: 6.18 to 8.43), Ecuador (7.17, 95% CI: 5.12 to 9.25), and Georgia (5.42, 95% CI: 4.89 to 5.95), contrasted by decreases in Greenland (−1.63, 95% CI: −1.78 to −1.48), Republic of Korea (−1.41, 95% CI: −1.70 to −1.11), and Bahrain (−1.03, 95% CI: −1.17 to −0.90) (Fig. 2B, Table S6). The geographical distribution of DALYs rates was basically similar to that of mortality rates, with increased EAPCs in Turkmenistan (6.95, 95% CI: 5.91 to 8.00), Ecuador (6.59, 95% CI: 4.58 to 8.64), and Georgia (4.90, 95% CI: 4.36 to 5.43), contrasted by decreases in Greenland (−1.83, 95% CI: −2.01 to −1.65), Republic of Korea (−1.47, 95% CI: −1.80 to −1.14), and Luxembourg (−1.41, 95% CI: −1.54 to −1.28) (Fig. 2C-D, Table S6).

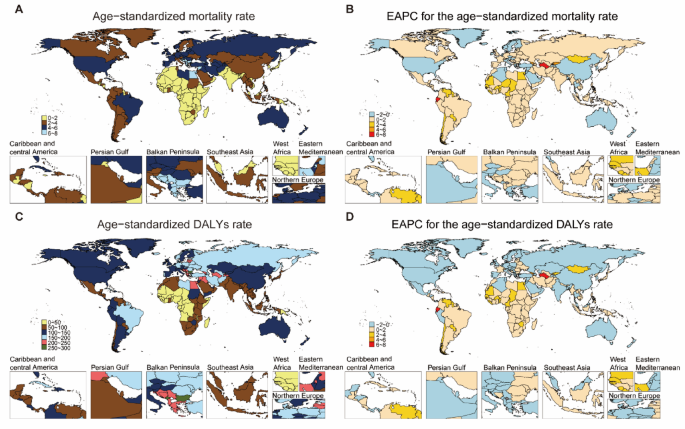
The Age-standardized Mortality and DALYs Rate of Brain and CNS Cancers in 204 Countries and Territories. (A) The ASMR of brain and CNS cancers in 2021. (B) The EAPC of ASMR of brain and CNS cancers from 1990 to 2021. (C) The ASDR of brain and CNS cancers in 2021. (D) The EAPC of ASDR of brain and CNS cancers from 1990 to 2021. ASMR age-standardized mortality rate, ASDR age-standardized DALYs rate, EAPC estimated annual percentage change, DALYs disability-adjusted life years.
Decomposition analysis of brain and CNS cancer burden
Between 1990 and 2021, the number of brain and CNS cancer incident cases increased from 173,086 to 357,482 across all SDI regions (Fig. 3A, Table S7). Population growth contributed the most to this increase with 98,494 additional cases, followed by aging with 55,337 cases, while epidemiological changes added 30,565 cases. The middle SDI regions experienced the largest absolute increase, adding 59,861 new cases during this period.

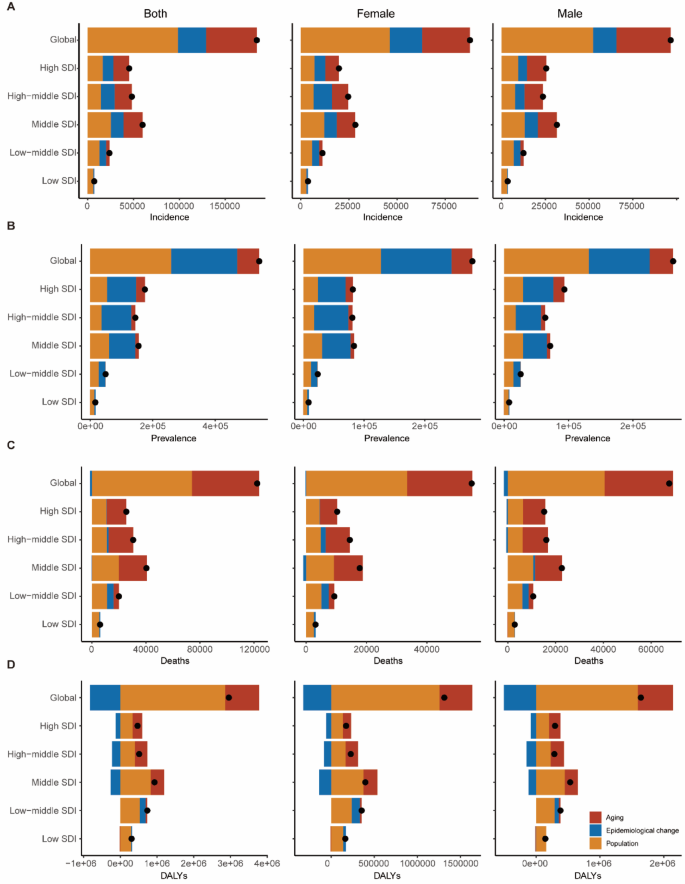
Changes in Burden of Brain and CNS Cancers from 1990 to 2021 at the Global Level and by SDI Quintile. (A-B) Changes in brain and CNS cancers incidence (A) and prevalence (B) according to population-level determinants of population growth, aging, and epidemiological change. (C-D) Changes in brain and CNS cancers deaths (C) and DALYs (D) according to population-level determinants of population growth, aging, and epidemiological change. The black dot represents the overall value of change contributed by all 3 components. For each component, the magnitude of a positive value indicates a corresponding increase in brain and CNS cancers DALYs attributed to the component; the magnitude of a negative value indicates a corresponding decrease in brain and CNS cancers attributed to the related component. SDI socio-demographic index, DALYs disability-adjusted life years.
Globally, there was substantial growth in the prevalence of brain and CNS cancers, with a rise of 540,856 cases (Fig. 3B, Table S8). The population growth accounted for 259,589 additional prevalent cases, while epidemiological changes and aging contributed 210,964 and 70,303 cases, respectively. High SDI regions experienced a notable pattern where epidemiological changes contributed 93,152 cases to prevalence.
Deaths from brain and CNS cancers exhibited an increase across in all SDI quintiles, with global deaths rising from 136,219 to 258,627 (Fig. 3C, Table S9). The primary drivers of this increase were population growth and aging, contributing 74,040 and 49,857 additional deaths, respectively, while epidemiological changes resulted in a slight reduction of 1,489 deaths. It is noteworthy that in low-middle SDI regions, the epidemiological component contributed 4,830 deaths, deviating from the global trend.
Concerning to DALYs, the global burden of brain and CNS cancers increased by approximately 3 million DALYs between 1990 and 2021 (Fig. 3D, Table S10). Population growth had the largest impact, adding 2,855,653 DALYs, while aging contributed 926,678 DALYs. Importantly, epidemiological changes reduced the DALYs burden by 828,217, partially offsetting the increases from demographic factors. However, similar to mortality patterns, in low-middle SDI regions, epidemiological changes actually increased the DALYs burden by 160,206, contrasting with the reductions seen in high, high-middle, and middle SDI regions.
Projections of future burden in the next 20 years
BAPC models were employed to forecast the burden of brain and CNS cancers through 2041, revealing notable patterns in projected trends by sex (Fig. 4). The findings of this study indicate a gradual decline in all metrics over the next two decades, with varying trajectories between females and males. For incidence rates, a decrease is projected for females from 3.874 ± 0.009 per 100,000 in 2021 to 3.387 ± 0.812 per 100,000 by 2041 (Fig. 4A, Table S11), representing a 12.6% reduction. A similar decline is predicted for male incidence rates, which are forecasted to decrease from 4.721 ± 0.011 to 4.060 ± 0.936 per 100,000 over the same period (Fig. 4A, Table S12), representing a 14.0% decrease. Prevalence rates demonstrate a comparable pattern of decline, with projections for females decreasing from 11.753 ± 0.017 to 10.200 ± 3.137 per 100,000. For males, the decline is projected to be from 12.269 ± 0.018 to 10.569 ± 3.253 per 100,000 by 2041 (Fig. 4B).

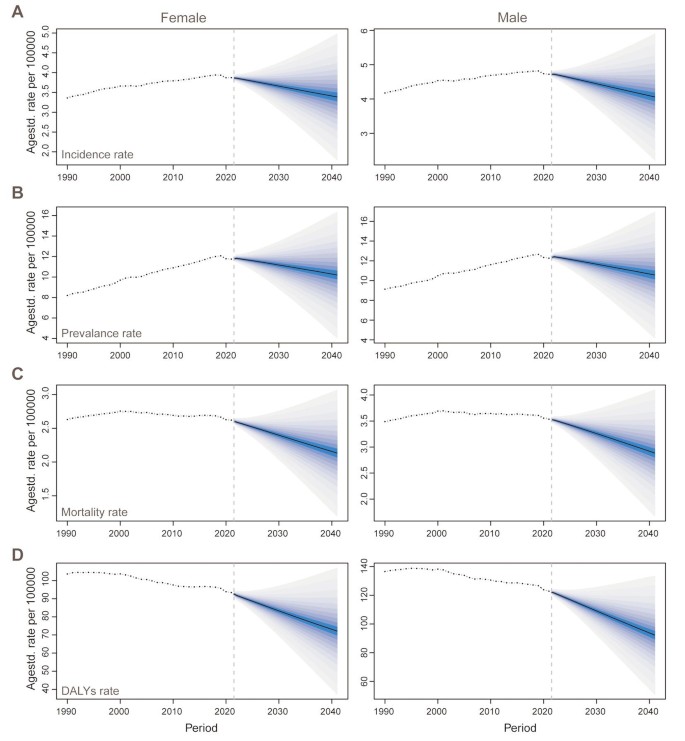
Trends and Projection for Brain and CNS Cancers by Sex from 1990 to 2041. (A-B) BAPC trends and projection for incidence rate (A) and prevalence rate (B) in females and males. (C-D) BAPC trends and projection for mortality rate (C) and DALYs rate (D) in females and males. BAPC Bayesian age-period-cohort projections, DALYs disability-adjusted life years.
Projections indicate a parallel decline in mortality rates, with female mortality rates anticipated to decrease from 2.620 ± 0.007 per 100,000 in 2021 to 2.133 ± 0.476 per 100,000 by 2041, representing an 18.6% reduction (Fig. 4C, Table S11). For males, the mortality rate is projected to decrease from 3.537 ± 0.009 to 2.885 ± 0.617 per 100,000, representing an 18.4% decline (Fig. 4C, Table S12). The most substantial reductions are projected for DALYs rates, with females expected to experience a 22.8% decrease from 93.390 ± 0.048 to 72.137 ± 17.723 per 100, 000, and males a 24.9% reduction from 122.878 ± 0.055 to 92.248 ± 20.945 per 100,000 (Fig. 4D, Table S12). Additionally, age-segmented forecasts reveal an important pattern in brain and CNS cancer burden through 2041 (Tables S13-20). Younger age groups are projected to experience substantial decreases in disease rates over time. Meanwhile, older populations aged 60 years and above will continue to have higher overall rates compared to younger groups, although their rates are also expected to decrease gradually from current levels.
link