
Lung function in adults born with very low birth weight from young to mid-adulthood

Study design
The data were collected with harmonized data collection and management procedures from two longitudinal birth cohorts; the Helsinki Study of Very Low Birth Weight Adults (HeSVA) in Helsinki, Finland and the NTNU Low Birth Weight in a Lifetime Perspective study (NTNU LBW Life) in Trondheim, Norway. The mid-adulthood follow-up visits were conducted in 2019–2021, including a respiratory health assessment by spirometry as part of an extensive health assessment.
The original HeSVA cohort has undergone detailed clinical assessment at ages 22 and 25 years. The cohort comprised 335 VLBW infants who were born between 1978 and 1985 and discharged alive from the neonatal intensive care unit of Helsinki University Central Hospital. For every VLBW infant was selected a term-born singleton infant of the same sex not born small for gestational age, group-matched for age, sex and birth hospital20,21. Lung function was examined in young adulthood during 2004–2005 by spirometry (Medikro) from 322 participants at a mean age of 22 years.7
The original NTNU LBW Life cohort have undergone detailed clinical assessment at ages 1, 5, 14, 18, 20, 23, and 26 years. The cohort comprised 88 VLBW infants who were born between 1986–1988 and discharged alive from the neonatal intensive care unit of St. Olavs Hospital, Trondheim, Norway. Control participants were recruited from a population-based multicenter study on causes and consequences of intrauterine growth restriction, where a 10% random sample was selected for follow-up during their mothers’ second or third pregnancy. Control participants were born at term and not small for gestational age in Trondheim region.22 Lung function was examined in young adulthood by spirometry (Sensormedics Vmax22 Encore) from 100 participants at mean age of 18 years.23
We combined and reanalyzed the young adulthood data from the HeSVA and NTNU LBW Life cohorts. The pooled young adulthood HeSVA-NTNU LBW Life dataset included altogether 423 participants at mean age 21.5 (SD 2.6) years; 110 VLBW women, 88 VLBW men, 129 control women and 96 control men (Fig. 1).
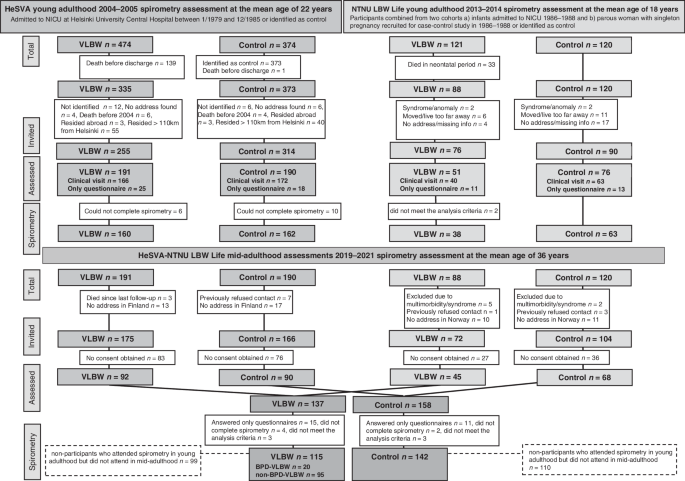
BPD bronchopulmonary dysplasia, HeSVA Helsinki study of very low birth weight adults, NICU neonatal intensive care unit, NTNU LBW Life NTNU low birth weight in a lifetime perspective study, VLBW very low birth weight.
Participants
The flow of study participants is described in Fig. 1.
A total of 175 VLBW adults from HeSVA and 72 from NTNU LBW Life were invited for mid-adulthood assessment at a mean age of 36 (SD 3.3) years and 137 participated (55.5% women). Of these, 15 answered questionnaires only and did not attend the clinical visits. Four participants were not able to complete spirometry due to technical reasons or having respiratory symptoms within the past two weeks before the clinical visit, and for three participants, spirometry values did not meet the reproducibility criteria.
In the spirometry analyses, we included 115 VLBW participants (59.1% women). Of these, 20 (60% women) had neonatal BPD and were included in the BPD-VLBW group, and 95 (58.9% women) participants without BPD were included in the non-BPD-VLBW group.
In our primary analyses, BPD was defined based on clinician’s diagnosis. In HeSVA, this was determined using the Northway criteria24 (respiratory distress, supplemental oxygen and characteristic radiographic findings at 1 month of postnatal age), all diagnoses confirmed by the same neonatologist, which has been used in our previous publications in HeSVA.7,25 For consistency, in NTNU, we used a clinician’s diagnosis collected from medical records. We also conducted sensitivity analyses using BPD definitions by the need for supplemental oxygen for more than 28 days (29 VLBW participants) and for more than 36 weeks (9 VLBW participants).
In the control group, 166 from HeSVA and 104 from NTNU LBW Life were invited and 158 (58.5% women) of them participated. Eleven control participants answered only questionnaires and did not attend clinical visits. Two control participants did not complete spirometry due to a shortage of staff. In the spirometry analyses, we included 142 control participants (57.7% women). Written informed consent was obtained from all participants who attended the study. The study protocols were approved by the ethics committee at the Helsinki and Uusimaa Hospital district (HUS/1157) and by the Regional Committee for Medical and Health Research Ethics in Central-Norway (23879). The protocol is registered as ISRCTN77533991.
Measures
In mid-adulthood, lung function was measured by spirometry (Medikro in HeSVA and Sensormedics in NTNU LBW Life). Spirometry was performed in accordance with the American Thoracic Society/European Respiratory Society recommendations.26 In HeSVA, the participants were instructed not to take their medication in the morning of the examination. In NTNU LBW Life, they were asked to continue their medication, including anti-obstructive medication, as usual. Reversibility tests were not performed. The devices were calibrated daily before measurements. Spirometry was not performed if the participant had had a respiratory infection in the past two weeks prior to the clinical visit. Spirometry was performed with participants in a sitting position wearing nose clips and holding mouthpiece tightly between teeth and lips. Respiratory volumes were standardized to barometric pressure at sea level and body temperature. The maneuver was repeated until three technically acceptable spirometry curves were obtained. The largest value of forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) were reported; the other measurements came from the maneuver where the sum of FVC and FEV1 was largest.26,27
Primary outcomes were FEV1 and ratio of the FEV1 to FVC (FEV1/FVC). Secondary outcomes were forced expiratory flow when 75% of FVC has been exhaled (FEF75%) and forced expiratory flow at 25–75% (FEF25–75%). All absolute values were converted to z-scores based on the Global Lung Function Initiative guidelines, which account for participant age, height, sex and race.28 Six participants were excluded from the analysis because they did not have (all) values for FEV1, FVC, FEV1/FVC or the values did not meet the reproducibility criteria according to American Thoracic Society and European Respiratory Society; for FEV1 and FVC the best two values had to be within 5% or 150 ml and for FEV1/FVC the difference of the sum of FEV1 and FVC had to be less than 300 ml. In addition, the participants answered the questionnaire on respiratory symptoms of the European Community Respiratory Health Survey.29 They were also asked to report the history of physician-diagnosed asthma and any regular or seasonal use of obstructive airway medication (ATC codes R03AC, R03AK, R03BA, R03DC).
Statistical methods and power calculation
The data were analyzed with IBM SPSS Statistics, version 29.0.0.0 (241). A priori power calculation was based on a total population of 170 VLBW participants and 200 controls. With a statistical power of 80% and an alpha level of 0.05, the detectable difference in a continuous outcome between groups was 0.29 SD score and with 90% power and an alpha of 0.01 the detectable difference was 0.40 SD. Before data analysis, with the actual number of 137 VLBW and 158 controls participants, the corresponding numbers were 0.33 and 0.45 SD.30
We assessed normality and distributions by evaluating histograms and Q–Q Plot residuals. The baseline characteristics comparisons between BPD-VLBW or non-BPD-VLBW groups and term-born controls were done by t-tests and X2 tests. To detect whether the associations between VLBW birth and lung function differed by sex, we added an interaction term group*sex for zFVC, zFEV1 and zFEV1/FVC both in young and mid-adulthood. We only found significant group*sex interaction in mid-adulthood zFVC. As FEV1 and FEV1/FVC absolute and z-score variables served as our primary outcomes, we decided to report the results for women and men together.
The most important modifier of the associations between VLBW birth and lung function and respiratory health was a history of BPD. Therefore, we present the results with lung function as an outcome, comparing the BPD-VLBW and non-BPD-VLBW groups with controls by linear regression models separately in young and mid-adulthood. All linear regression analyses were adjusted for cohort, age and sex (model 1). In further adjustments, model 2 included, in addition highest parental educational attainment and model 3 highest parental educational attainment and maternal smoking. Model 3 was conducted only for HeSVA participants because NTNU LBW Life did not have data on maternal smoking in pregnancy. We used mixed model analysis to estimate whether the BPD-VLBW or non-BPD-VLBW participants would have a faster rate of decline in spirometry outcomes between young and mid-adulthood, as compared with controls. To do so, we added an interaction term “group (BPD-VLBW or non-BPD-VLBW vs. control) * assessment timepoint (young vs. mid-adulthood)” in the model that also included the main effects of the group and assessment timepoint, as well as cohort, sex and age at young adulthood assessment.
In addition, using the same methods, we conducted an analysis between BPD-VLBW and non-BPD-VLBW participants to assess differences within the VLBW group, adjusting for model 1 variables. As a further sensitivity analysis, we compared BPD-VLBW population spirometry outcomes with controls by defining BPD by the need for supplemental oxygen for more than 28 days or for more than 36 (postmenstrual) weeks.
To compare dichotomous outcomes, including respiratory symptoms or a history of obstructive airway disease, between the VLBW and control groups, we used logistic regression.
To estimate possible effects of the participant’s smoking on respiratory health we performed linear regression (adjustment model 1) in each time point within and between the VLBW and control participants who had reported their smoking status in the mid-adulthood visit questionnaire and had spirometry data available from both assessment points (n = 209) allowing age interaction to be assessed by mixed models. We conducted a dichotomous variable indicating whether the participant had any kind of smoking history compared with those who had never smoked. We conducted the comparisons between VLBW and control participants with smoking history and within the VLBW and control groups with or without smoking history.
link



